We understand that making sure you know what to expect from your joint replacement experience is important to you. As you are reading through this material, if you have additional questions please reach out to us to discuss.
 Each patient is unique, and can experience joint pain for different reasons. It’s important to talk to us about the reason for your joint pain so you can understand the treatment options available to you. Pain from arthritis and joint degeneration can be constant or come and go, occur with movement or after a period of rest, or be located in one spot or many parts of the body. It is common for patients to try medication and other conservative treatments to treat their hip or knee pain. If you haven’t experienced adequate relief with those treatment options, you may be a candidate for Mako Total Hip, Total Knee or Partial Knee replacement, which may provide you with relief from your joint pain.
Each patient is unique, and can experience joint pain for different reasons. It’s important to talk to us about the reason for your joint pain so you can understand the treatment options available to you. Pain from arthritis and joint degeneration can be constant or come and go, occur with movement or after a period of rest, or be located in one spot or many parts of the body. It is common for patients to try medication and other conservative treatments to treat their hip or knee pain. If you haven’t experienced adequate relief with those treatment options, you may be a candidate for Mako Total Hip, Total Knee or Partial Knee replacement, which may provide you with relief from your joint pain.
How Mako Technology works
Mako Robotic-Arm Assisted Technology provides you with a personalized surgical plan based on your unique anatomy. First, a CT scan of the diseased hip or knee joint is taken. This CT scan is uploaded into the Mako System software, where a 3D model of your hip or knee is created. This 3D model is used to pre-plan and assist your surgeon in performing your joint replacement procedure.
In the operating room, your surgeon follows your personalized surgical plan while preparing the bone for the implant. The surgeon guides the robotic-arm within the pre-defined area and the Mako System helps the surgeon stay within the planned boundaries that were defined when the personalized pre-operative plan was created. In a laboratory study, Mako Total Knee Technology demonstrated accurate placement of implants to a personalized surgical plan.1 This study also showed that Mako Total Knee replacement demonstrated soft tissue protection to the ligaments around the knee.1In patient and laboratory studies on Mako Total Hip and Partial Knee replacement, Mako Technology demonstrated accurate placement of implants to a personalized surgical plan.2-4
Total knee vs. partial knee replacement
Based on the severity of the arthritis in the knee, total or partial knee replacement may be recommended by a surgeon. Both procedures involve the orthopaedic surgeon guiding the Mako Robotic-Arm to remove diseased bone and cartilage.

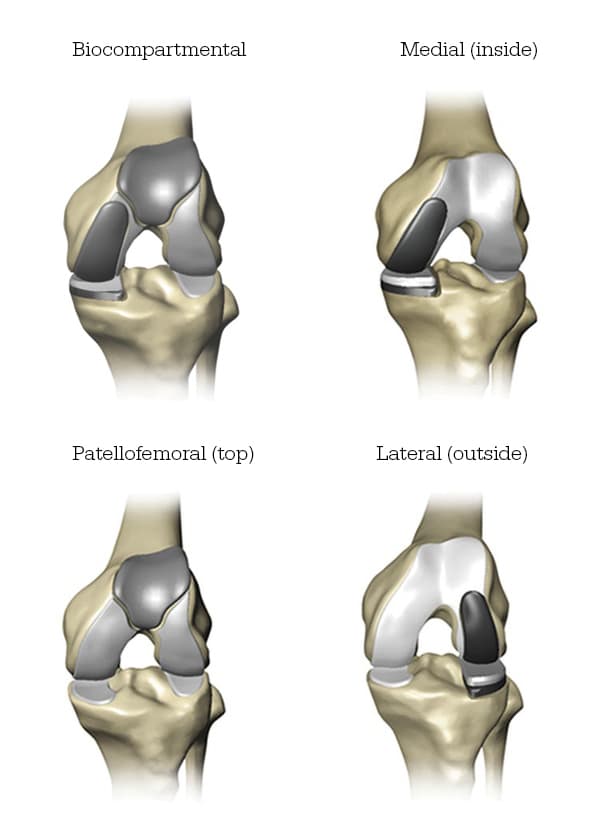
- Mako Robotic-Arm Assisted Partial Knee replacement is a treatment option for adults living with early to mid-stage osteoarthritis (OA) that has not yet progressed to all three compartments of the knee. Depending on where the arthritis affects the knee, patients may have an implant inserted in any of the following areas:
Step 1. Knee CT Scan

Step 2. Knee Personalized Planning

- In comparison, Mako Robotic-Arm Assisted Total Knee replacement is a treatment option for adults living with mid to late-stage osteoarthritis of the knee. With Mako Total Knee replacement, the entire knee joint is replaced and the surgeon inserts a Triathlon Total Knee implant. With over a decade of clinical history, Triathlon knee replacements are different than traditional knee replacements because they are designed to work with the body to promote natural-like circular motion.5-8
Step 1. Knee CT Scan
Step 2. Knee Personalized Planning

Stryker Corporation or its other divisions or other corporate affiliated entities own, use or have applied for the following trademarks or service marks: Mako, Stryker, Triathlon. All other trademarks are trademarks of their respected owners or holders.
References
- Nawabi DH, Conditt MA, Ranawat AS, Dunbar NJ, Jones J, Banks SA, Padgett DE. Haptically guided robotic technology in total hip arthroplasty – a cadaver investigation. Proc Inst Mech Eng H. 2013 Mar22 7(3):302-9
- Illgen R. Robotic assisted total hip arthroplasty improves accuracy and clinical outcome compared with manual technique. 44th Annual Advances in Arthroplasty Course. October 7-10, 2014, Cambridge, MA.F
- 1. Bell, Stuart W. MBChB, MRCP, FRCS(T&O), Anthony, IainPhD, Jones, Bryn MBChB, FRCS(T&O), MacLean, Angus MBChB, RCS(T&O), Rowe, Philip BSc(Hons), PhD, and Blyth, Mark MBChB, FRCS(T&O). Improved accuracy of component positioning with robotic-assisted unicompartmental knee arthroplasty. The Journal of Bone and Joint Surgery. Volume 98-A: Number 8. April 20, 2016. pp 627-35.
- Bell, Stuart W., Anthony, Iain, Jones, Bryn, MacLean, Angus, Rowe, Philip, and Blyth, Mark. Improved accuracy of component positioning with robotic-assisted unicompartmental knee arthroplasty. The Journal of Bone and Joint Surgery. Volume 98-A: Number 8. April 20, 2016. pp 627-35.
- Mistry J, Elmallah R, Chughtai M, Oktem M, Harwin S, Mont M. Long-Term Survivorship and Clinical Outcomes of a Single Radius Total Knee Arthroplasty. International XXVIII.
- Designed to maintain collateral ligament stability throughout the range of motion. Stryker-Initiated Dynamic Computer Simulations of Passive ROM and Oxford Rig Test, Stephen Piazza, 2003.
- Wang H, Simpson KJ, Ferrara MS, Chamnongkich S, Kinsey T, Mahoney, OM. Biomechanical differences exhibited during sit-to-stand between total knee arthroplasty designs of varying radii. J Arthroplasty. 2006;21(8):1193-1199.
- Gómez-Barrena E, Fernandez-García C, Fernandez- Bravo A, Cutillas-Ruiz R, Bermejo-Fernandez G. Functional performance with a single-radius femoral design total knee arthroplasty. Clin Ortho Relates Res. 2010;468(5):1214-1220.
MKOHMT-PE-3_Rev-1_13841 Copyright © 2017 Stryker Corporation